[HAWAII AT WORK]
DENNIS ODA / DODA@STARBULLETIN.COM
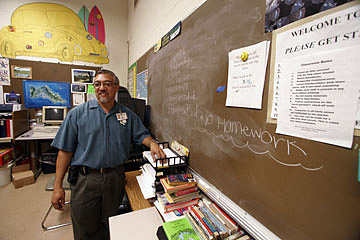
Youths with chronic behavioral problems sometimes are assigned to Kahi Mohala's acute adolescent treatment program in Ewa, where lead teacher Frank Dumlao, above, helps them keep up with their regular schooling and tries to help them see life from a different point of view. CLICK FOR LARGE
|
|
Offering a new perspective
Frank Dumlao helps troubled kids find the right tools to deal with their issues
FRANK Dumlao tries to help troubled kids get a grip by encouraging them to see the world the way it is, not the way they want it to be.
HAWAII AT WORK
Who: Frank Dumlao
Title: Lead teacher
Job: Teaches students with behavioral issues who have been assigned to Kahi Mohala
|
Dumlao is the lead teacher at Kahi Mohala, a nonprofit, licensed medical center off Old Fort Weaver Road in Ewa, operated by Sutter Health, of California, that specializes in behavioral health care. Dumlao works mostly with kids in grades 6 to 12, helping them keep up with their schoolwork while they stay at the center.
Before joining Kahi Mohala 22 years ago, Dumlao taught autistic and mentally retarded children at the Special Education Center of Oahu. It was the Waipahu High School graduate's first job after obtaining a degree in music education therapy from the University of Kansas.
While working for at the center, Dumlao also obtained a special education diploma from Brigham Young University-Hawaii. Later, he also obtained a master's degree in education from Central Michigan University.
Dumlao, 51, is married to the former Claire Chinen, with whom he has a 17-year-old son and lives in Kapolei.
Question: What does it mean that you're the lead teacher? Are there other teachers there and you're their supervisor?
Answer: There's actually just one other teacher. (Laughter) We used to have more, when we had more kids, so that's when I became the lead teacher, because I'm just old. (Laughter) I've been here the longest.
Q: How long have you been there?
A: Since 1984. So that's more than 20 years. When the trees were 10 feet tall.
Q: How tall are they now?
A: Oh, they're maybe 60 feet. They're eucalyptus trees.
Q: What was your first position there?
A: Same thing. I was teaching. I've always been in a teaching position here. I kind of helped developed the program.
Q: What is the program exactly?
A: I provide the educational component in the residential treatment program here. So I coordinate with the home schools and with the patients.
Q: Home schools -- you mean home schooling?
A: No, the public schools or wherever. That refers to wherever they're enrolled in, because they don't enroll here.
Q: If they're enrolled somewhere else, why are they at Kahi Mohala?
A: They have different mental health issues that cause them to need this level of care.
DENNIS ODA / DODA@STARBULLETIN.COM
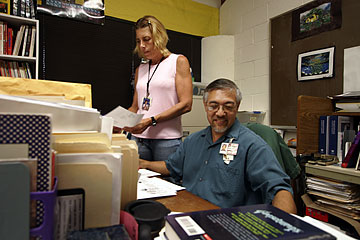
Frank Dumlao sometimes teaches class with the help of mental health specialists. In class last week, Dumlao, right, was assisted by Kathy Hanson, left, and Jesse Garcia, not shown.. CLICK FOR LARGE
|
|
And what kind of care is that?
A: Residential means 24/7, so every part of their life is in a therapeutic environment, including the classroom. So based on their issues, whatever it is, that's how we individually address their behaviors and attitudes.
Q: Do they live there?
A: Yes.
Q: For how long?
A: It varies, but usually one to three months. And it depends on where they're going to go next, whether they're going to go home or onto other living arrangements, like foster care, a group home or community-based care -- moving up the level of care.
Q: How does one get assigned to Kahi Mohala?
A: It's a medical referral, through the (state) Department of Health. They refer a patient, and it goes through our process here. A doctor is assigned, and a doctor would put a referral in for his or her care, a psychiatrist.
Q: Is this an alternative to juvenile detention?
A: No, because this is a hospital. We have therapeutic approaches. It's not punitive.
Q: Are the kids cooperative?
A: (Laughter) Depending on how you mean cooperative. They come in. But most of the kids, they have mental health issues, so depending on what brought them here, they're motivated toward the therapy. And there's a criteria in general, that the treatment team looks at. That (the team) includes the doctor, the clinical therapist, the nursing staff, myself in education, and occupational therapy.
Q: What is the average age of the students you work with?
A: We can go from K to 12. For myself, I see the secondary kids, from grades 6 to 12.
Q: And what do you do specifically for them?
A: Again, I coordinate with the home school regarding what courses they're enrolled in. And I cover the core courses: language arts, math, social studies and science. It's like a one-room school house. That's how I describe it to people who are trying to visualize what it's like. And it's individualized, so a kid could be in basic math while another is in algebra or pre-calculus -- the whole gamut.
Q: So I guess that means you know stuff like calculus.
A: Well, it doesn't mean that I know that. (Laughter). I really utilize, sometimes, the staff for the higher-level courses, because I figure somebody here must have taken those kinds of courses. But generally the kids must be pretty smart themselves if they're taking those courses.
Q: How many students do you teach each day?
A: It varies, I can go up to about eight to 10. But just to clarify, I can go eight to 10, but they're more focused on themselves, so occasionally I'll throw in a group activity, to see how they react to their peers, how they tolerate waiting, how they tolerate me. (Laughter) It's a whole different ballgame.
Q: So you're teaching, like, 10 kids all individually at the same time?
A: Right, but it's a positive thing. And one thing I like about the program is that we try to supply class materials and supplies that are up to date. It can be very expensive.
Q: Do you bond with these kids at all?
A: Oh yeah. I think developing a relationship is the key to getting results, that therapeutic relationship.
Q: And how do you do that?
A: Just talking to these kids, knowing their issues, being part of the developing team, trying to get their trust. Sometimes they're unreachable or more challenging, but I think one of the good things about my situation is that every one of these kids has gone to school, so they have some concept of schooling. There are some expectations that they have already. They see a desk, they know what to do with it.
Q: What kinds of issues do you deal with?
A: Kids that have depression, conduct disorder, eating disorder, other psychiatric psychoses, substance problems -- substance is a big thing. And it's just compounded because there are family issues that go with that, and social issues, because it's in the court system. By the time that they hit the older age, the ninth-grade, there's a lot of stuff that's been built up. So I'm trying to teach them some perspective.
Q: Do you ever talk to them about how to avoid getting sucked into the system?
A: Yes, that's a big thing that we talk to them about.
Like some kid may be in here because of anger, and I'm the teacher, and they may take it out on me, or other authority figures, so what I do is teach them some perspective.
And a unique thing is, I can address their mental health issues at the same time I address how their mental health issues have impacted their goals in school, their future, and how their perception of school can play into their future goals. Within a certain period of time, I try to give them some tools to put into their tool box. Some kids are trying to turn the screw with a hammer.
At the same time, I'll have a student who may not accept their learning disabilities, whether it be in reading or writing, like with attention deficit -- that's a big thing: attention deficit disorders.
Q: How do you address that?
A: With medicine (as prescribed by the doctors),* but in terms of what I do, along with the medicine, I just label the behavior and give them alternative behaviors that are more appropriate.
Q: In terms of the medicine, how much of a role does that take?
A: Whatever the doctor prescribes, I just understand that the kid is on a medication, and I just try to see if there is a difference in terms of his attention, his reaction. For example, if a kid comes in here and the issue is he overreacts to correction, and they blow up, then the doctor puts him on some medication, and if he doesn't do it anymore or his frustration level/ tolerance level increases, then I report that.
I look for other things too, including whether family issues are improving.
Q: Is there a particular socio-economic background you're dealing with?
A: They vary. But whether they come from poor families or well-to-do families, they're the same. In fact, I don't see it as an issue of whether they have everything in life. It comes down to what they see the world as.
Q: So are you pretty happy working at Kahi Mohala?
A: Oh yeah. People ask me why I've been here so long. But it's a career. I enjoy it.
CLARIFICATION
Wednesday, December 20, 2006
» In Monday's "Hawaii at Work" interview on Page C1 with Frank Dumlao, lead teacher at Kahi Mohala, the morning edition had Dumlao responding to the question "How do you address that?" (referring to students with attention deficit disorders) with the answer, "With medicine ..." The afternoon edition added "(as prescribed by the doctors)" to make clear that Dumlao is not the one who prescribes or administers the medicine.
|

