ASSOCIATED PRESS
Dr. David Reuben, left, chief of geriatrics at the University of California at Los Angeles School of Medicine, consults with patient Olive Rolnick, 91. Across the country, including Hawaii, doctors are choosing to pursue specialties other than geriatrics, even as the general population ages.
Few isle doctors Lisa Skinner, a chief resident at UCLA School of Medicine, thought about specializing in the treatment of old people, and even got a master's degree in geriatric social work. In the end, she opted to pursue general internal medicine.
specialize in elder care
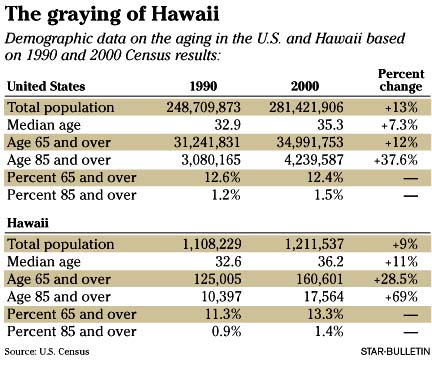
Baby boomers are aging, but
MDs shy away from geriatricsStar-Bulletin staff and wire
"I hated to give up the younger patients, even though I enjoy the older patients," she said.
Across the country, thousands of new doctors like Skinner have decided to pursue specialties other than geriatrics, a trend that has created a vast shortage of elder care doctors.
In Hawaii, it's a similar story. There are 20 geriatric specialists, called geriatricians, statewide according to Dr. Patricia Lanoie Blanchette, University of Hawaii Geriatric Medicine Program director. That number has dropped from about 25 in 2001. Most are either staff physicians employed by hospitals or university faculty. Just one is in private practice.
Experts who worry about the depth of the problem say it's going to become extreme when baby boomers start hitting old age -- creating a "senior boom" -- and start needing special care.
"It's going to be enormous," said Dr. David Reuben, chief of geriatrics at the University of California at Los Angeles, School of Medicine. "You can't imagine how big this is going to be."
Reuben is one of the 76 million Americans born between 1946 and 1964, known collectively as baby boomers. "In 2011, we're going to start hitting 65. One of out every five people in the country," he said.
He and other experts say baby boomers probably aren't worrying about geriatric issues right now -- unless they have sick parents.
"It's a problem that the baby boomer generation is seeing now as they see the quality of care for their parents," said Daniel Perry, executive director of the Alliance for Aging Research. "They're coming away from that experience confused, seeing their parents passed from one physician to another."
At least 20,000 geriatricians are needed to care for the 35 million Americans over age 65, according to the alliance, a nonprofit advocacy group. But only 9,000 out of the 650,000 doctors in this country are certified in geriatric medicine. "It's one of the great disconnects in American health care," Perry said.
And future geriatricians aren't coming down the pipeline. Of the 126 accredited medical schools in the United States, only three have a geriatrics department, says the Association of American Medical Colleges. The rest cover elder care within broader classes.
Every year, about 16,000 students graduate from U.S. medical schools, with another 7,500 coming from abroad. Out of those 23,500 newly minted doctors, only about 500 -- or 2 percent -- go into geriatrics.
Right now, geriatricians are primarily hired by hospitals and universities so they can either teach geriatric medicine or consult for a large medical center.
With such a shortage, recruiting geriatricians is difficult -- and competitive, UH's Blanchette said.
Moreover, insurance reimbursements, primarily from Medicare and Medicaid, make it difficult for anyone considering geriatrics as a private practice, Blanchette said.
An examination of an elderly patient newly admitted to a nursing home would likely take the attending physician a couple of hours, said Blanchette. And the average patient would likely have several illnesses or underlying conditions, there would need to be a complete review of the patient's existing medical records, multiple phone calls and lots of paperwork would be required. For that visit, Medicare would pay $104.48, she said.
"(Geriatrics) is the lowest paid specialty in terms of reimbursements. So the more Medicare patients you have, the less viable your practice. So in the fee-for-service world, it just doesn't work," she said.
That's why most geriatricians turn either to teaching in a university or working for a large health care organization, where they consult with other physicians on their elderly patients or see only the most complicated patients.
UH's John A. Burns School of Medicine has received several grants that may help improve the situation.
It received $2 million grant from the Donald W. Reynolds Foundation and a $450,000 three-year renewal grant from the John A. Hartford Foundation in 2001 that is being used to ease the shortage in academic geriatricians.
Many experts believe the best -- and possibly only -- solution may be to train all physicians, regardless of their specialty, in aspects of geriatrics related to their field. That is happening at UH, Blanchette said.
"We have a fellowship program which takes MDs already trained in family practice or internal medicine and trains them for one year to become a specialist in geriatric medicine," she said.
Medical students are also receiving more training in geriatrics now, just as they receive training in specialties such as pediatrics, regardless of whether they intend to specialize in that area.
"It's well under way. We're already training students in all four years of medical school," she said.
In addition, graduates who are already going through various residency programs get some specialized training in geriatrics related to their particular discipline.
"So, for example in surgery, you would teach a resident to take better care of an older person in that area," she said.
Still, Blanchette said, more has to be done to encourage people to specialize in the field.
Improved reimbursements would be one positive step, she said.
"Something has to be done in terms of changing Medicare reimbursements. At one time, you could provide some free care when reimbursements from other insurers were better. Now it's more difficult," she said.
Partial forgiveness of loans for medical students willing to specialize in the field would be another.
The public also needs to become more familiar with the kinds of services a geriatricians provide, she said. For example, most people are confused between the terms geriatrician and gerontologist and use them interchangeably, said Blanchette.
While a geriatrician is a physician who specializes in care of the elderly, a gerontologist is a scientist who is trained in the study of aging. How they apply that knowledge depends on their area of interest or discipline.
Blanchette notes there was the same lack of knowledge in the 1930s when pediatric medicine was first recognized. Pediatrics came about in part because people began to view children differently, she said.
"At that time there was a combination of factors that led to the development of pediatrics," she said. "People recognized that you can't treat children like adults. There was also a social pressure, a different view of childhood where children were no longer expected to work."
Such a change in thinking is what is needed when it comes to the elderly, Blanchette said.
"It turns out now that what we are seeing with the elderly is that there may be a different view of aging, that certain things are not inevitable that you can have a healthier old age," she said.
Star-Bulletin reporter Lyn Danninger and the Associated Press contributed to this story.